How Predictive Diagnostics and AI Can Prevent the Collapse of Reactive Health Systems
The United States spends more on health care than any nation on earth and ranks last among wealthy countries in years of healthy life. The failure is architectural, not financial—and a four-level model offers a way to correct it.
By Camillo Ricordi, M.D.
The $5.3 Trillion Paradox
The United States spends roughly $5.3 trillion a year on health care—about 18% of gross domestic product, and more than any other nation on earth. By the measure that should matter most, the return on that expenditure is dismal. Among high-income countries, the U.S. ranks near the bottom in healthspan: the number of years its citizens can expect to live in good health, free of disabling chronic disease. After age 65, roughly nine in ten Americans live with at least one chronic condition, and most live with several. This is not a paradox of insufficient funding. It is evidence that a health system can fail even when resources are abundant—because the decisive question is not how much is spent, but on what, and when.
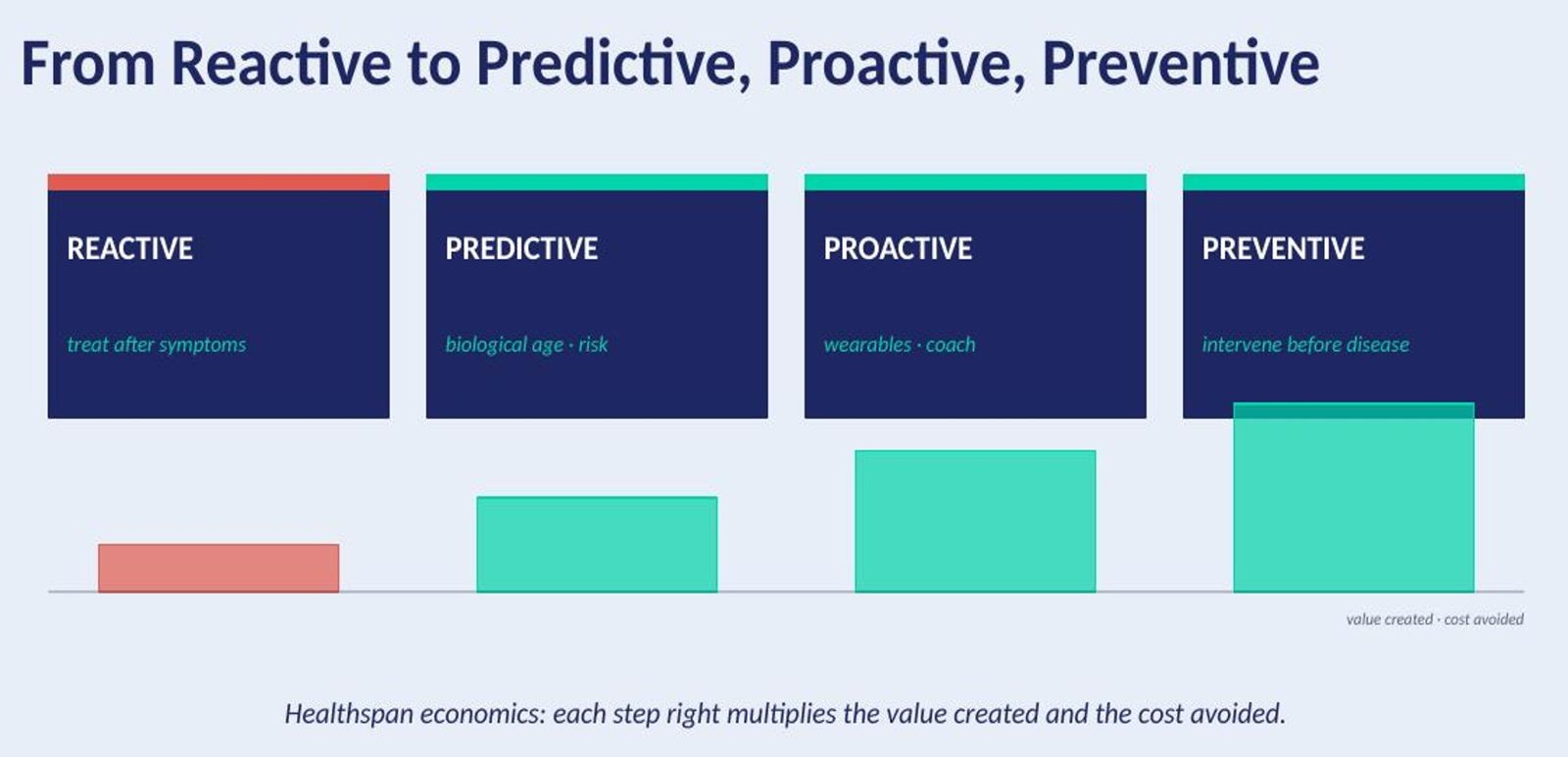
A System Built to React
The root of the problem is architectural rather than financial. American medicine, like most of Western medicine, is engineered to react. It activates at the moment a patient falls ill and almost never before. That design was rational when the dominant threats to life were acute: infections, injuries, the sudden catastrophe of a heart attack. It is profoundly mismatched to the crisis that now defines morbidity in wealthy nations—a slow-motion epidemic of chronic disease that develops silently over years and decades, driven by the gradual and largely invisible accumulation of metabolic, vascular, and inflammatory damage. By the time such a process announces itself as a diagnosis, the damage is often advanced and, in many cases, irreversible.
The Scale of What Is Coming
Diabetes illustrates the trajectory, and it is only the tip of the iceberg. The world had roughly 171 million cases in 2000. Today it has 589 million, and the International Diabetes Federation projects 853 million by 2050. The demographic current beneath these numbers is just as consequential: the global population over 60, among whom chronic disease concentrates, will nearly double within the coming two decades. Each of those diagnoses arrives years—often a decade or more—after the underlying derangement began. A purely reactive system meets every one of these patients at the worst possible moment: late, expensive, and frequently past the point of reversal. Adding more physicians, hospitals, and drugs to such a system, without changing its logic, is like applying fresh bandages to a wound that never heals.
Spending More, Living Less
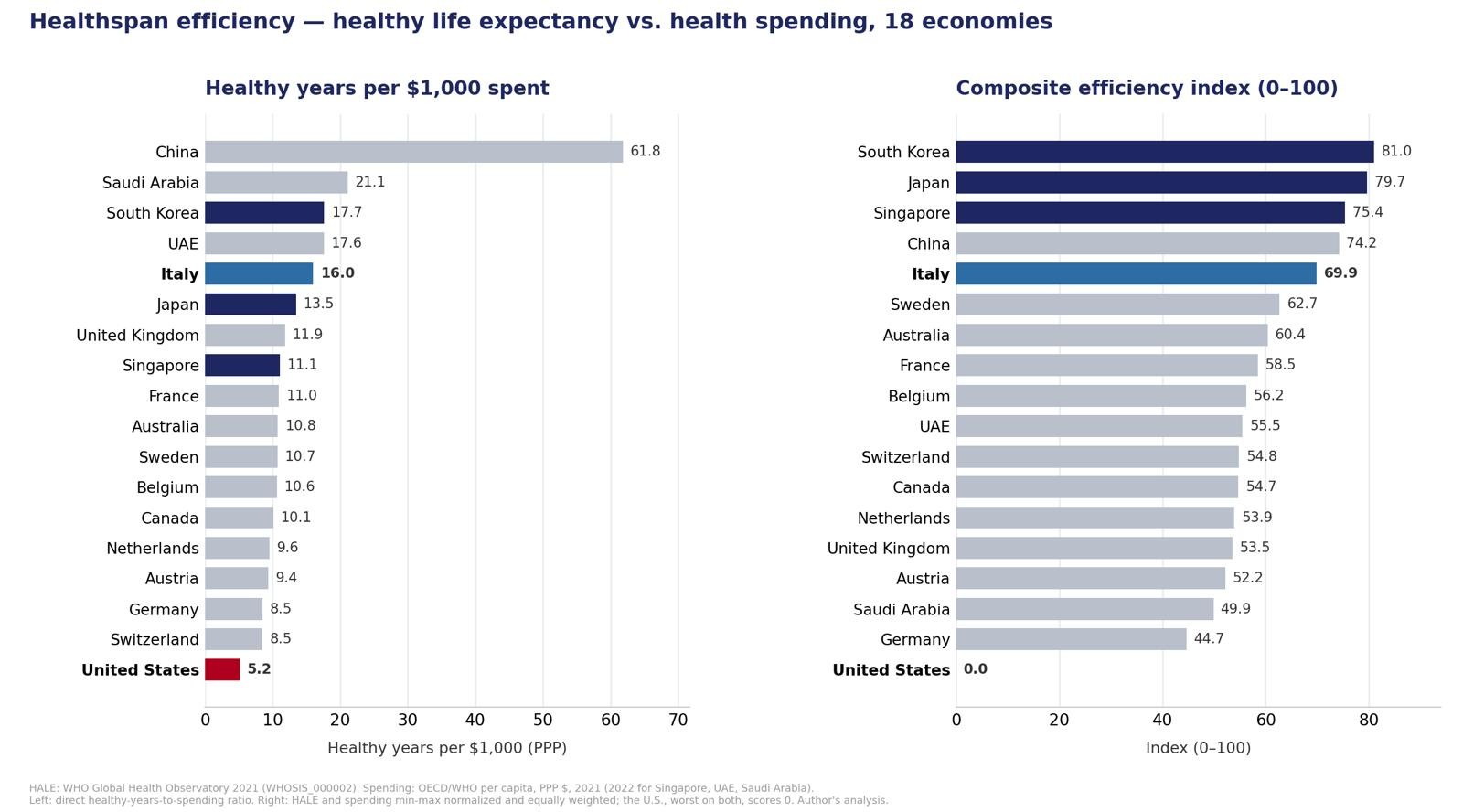
The clearest way to see the failure is to weigh what nations spend against the health they obtain. Combining the World Health Organization's most recent healthy-life-expectancy (HALE) estimates with health spending per capita (OECD and WHO data, in purchasing-power-adjusted dollars), one can construct a simple efficiency index across eighteen high-income and major economies: normalize each country's healthy years and its spending, weight the two equally, and score how much health each dollar buys.¹ʲ The result is stark.
The United States finishes dead last. It spends more than any nation on earth and, on the latest available figures, records among the fewest healthy years of any wealthy nation. The most efficient systems are in East Asia—South Korea, Japan, and Singapore lead—achieving the longest healthy lives at roughly a third of U.S. per-capita spending. Italy is the highest-ranked Western nation and the only one in the top five, converting modest expenditure into among the longest healthspans measured. The common thread among the leaders is not that they spend more; several spend a fraction of what the United States does. It is that they intervene earlier—on nutrition, lifestyle, and risk—before disease takes hold. The lesson is not that America is uniquely incapable, but that money deployed inside a reactive architecture buys remarkably little health, while comparatively modest investment in prevention buys a great deal.
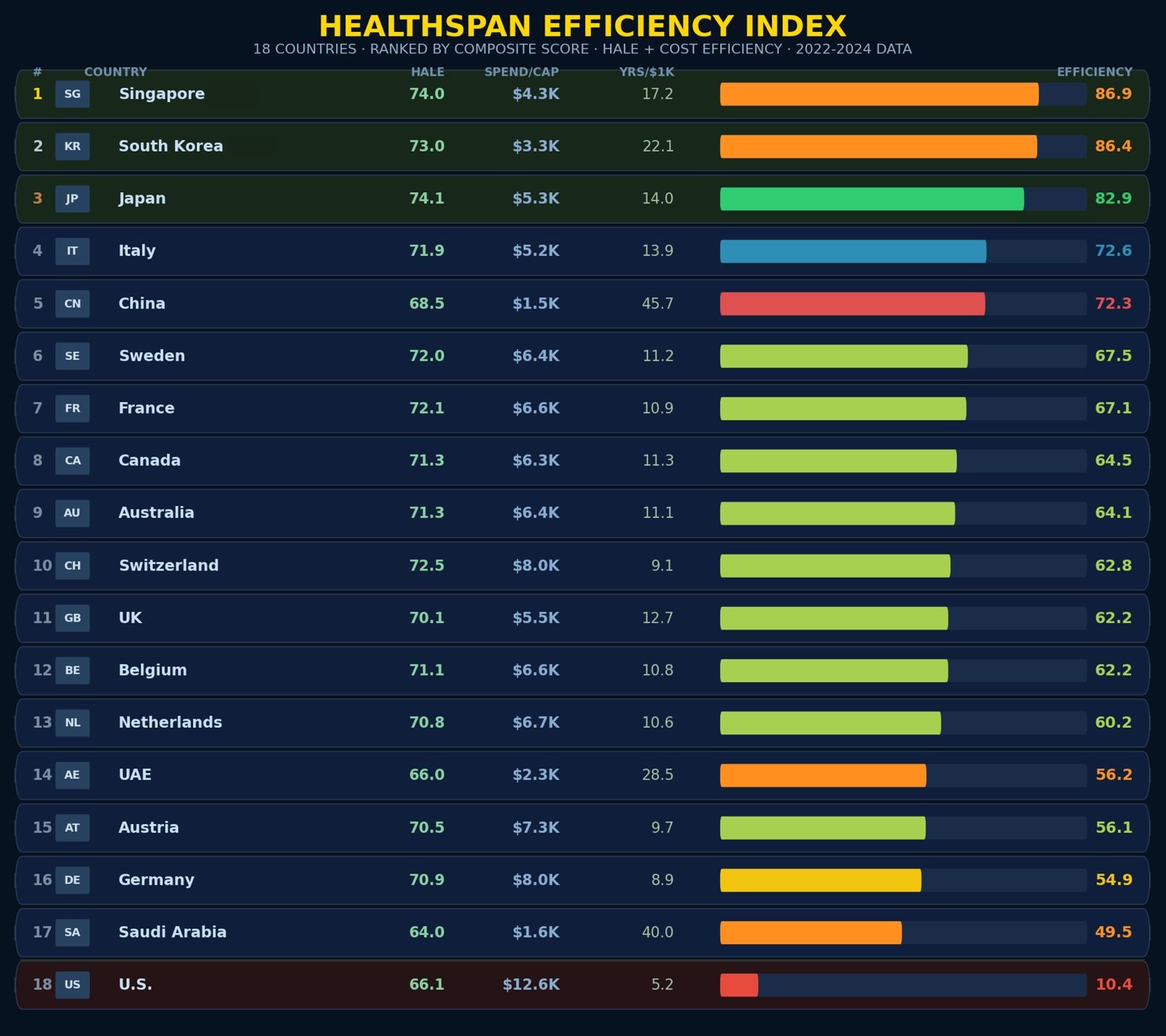
Figure 1. Healthspan Efficiency Index. Eighteen major economies ranked by a composite score that normalizes each country’s healthy life expectancy (HALE) and health spending per capita and weights the two equally, measuring how much health each dollar buys. Singapore, South Korea, and Japan lead, achieving the longest healthy lives at roughly a third of U.S. per-capita spending; Italy is the highest-ranked Western nation and the only one in the top five. The United States finishes last, pairing the group’s highest spending (~$12.6K per capita) with one of its lowest healthspans. HALE: WHO Global Health Observatory. Spending: OECD Health at a Glance and the WHO Global Health Expenditure Database, purchasing-power-adjusted. Author’s analysis (Refs. 1, 2).

Figure 2. Healthy Years per $1,000 Spent. The same eighteen countries ranked by a raw value ratio—healthy life-years (HALE) divided by health spending per capita in thousands of purchasing-power-adjusted dollars. This unweighted view rewards low spenders most: China, Saudi Arabia, and the UAE lead on cost alone, while the East Asian systems remain strong once absolute healthspan is also considered (Fig. 1). The United States again ranks last, returning just 5.2 healthy years per $1,000 spent—less than half the next-lowest country. Sources as in Fig. 1.

Figure 3. Healthspan (HALE) Ranking. The eighteen countries ranked solely by healthy life expectancy at birth, in years, independent of cost. Japan (74.1), Singapore (74.0), and South Korea (73.0) lead; the United States (66.1) sits near the bottom despite spending far more than any nation above it—the gap between health achieved and money spent that Figures 1 and 2 quantify. HALE: WHO Global Health Observatory (Ref. 1).
Healthspan Engineering: Four Connected Levels
It is possible to engineer healthy longevity—Healthspan Engineering—without dismantling the advanced, intervention-heavy medicine at which the United States excels. Doing so means enclosing that medicine within a system designed to protect health rather than merely to treat disease. That system can be understood as four connected levels, joined by a common thread of predictive information.
Level One: Seeing Risk Before Disease
The first level is predictive diagnostics: the capacity to detect elevated risk long before it manifests as illness. A generation ago, characterizing a person's biological trajectory required a hospital laboratory and a battery of separate tests. Increasingly, a single drop of blood can yield a multidimensional readout of the processes that drive accelerated aging and chronic disease—markers of glucose regulation and insulin resistance, lipid subfractions, chronic low-grade inflammation (the phenomenon researchers term inflammaging), and molecular signatures that estimate the biological, as distinct from chronological, age of the body and its organs. Individually, few of these measures are new. What is new is the capacity to assess many of them together, inexpensively, and to interpret them as a whole.
That interpretation is where artificial intelligence becomes decisive. No clinician can hold thousands of interacting variables in mind, nor track how they drift over time across millions of patients. Machine-learning models can. Trained on large longitudinal datasets, they can recognize the patterns that precede metabolic, cardiovascular, and neurodegenerative disease—often years in advance—and translate a static snapshot into a trajectory: not merely where a person stands today, but where they are heading, and how quickly. Used rigorously, this transforms medicine from a discipline that names diseases after they arrive into one that anticipates them while they can still be averted.
Level Two: Reversing the Trajectory
The second level is early intervention: acting on those signals to halt and, where possible, reverse progression while it remains inexpensive and reversible. The window is everything. Prediabetes can frequently be reversed; established type 2 diabetes is generally managed for life. Early arterial inflammation can be quieted; a completed myocardial infarction cannot be undone. The vast human and economic gulf between these two moments—catching a process on the way up, versus treating its consequences on the way down—is the ground on which the entire case for prevention stands.
Level Three: Treating Those Already Sick
The third level is advanced treatment for those already ill. Prevention, however effective, will never reach everyone in time; some people arrive already sick, and a credible, humane system leaves none of them behind. Here the United States possesses genuine and hard-won strengths—a formidable research base, world-leading surgical and pharmaceutical capabilities, and pioneering cell and gene therapies. Nothing in the healthspan model asks the country to weaken these capacities. The argument is that they should function as the last line of defense rather than the first and only one, and that dramatically reducing the largely preventable volume of patients who reach this level is precisely what would make it sustainable.
Level Four: Preventing Recurrence
The fourth level is the prevention of recurrence. A successful treatment is not the end of the story; without vigilance, disease returns and the reactive cycle begins anew. This lesson is written most vividly in the fields where cure is a literal ambition. In transplantation and in oncology, restoring a patient to health is only the beginning of a sustained effort to keep them there—through continuous monitoring, early detection of relapse, and reinforcement of the conditions that sustain remission. The same discipline applies to chronic disease reversed at the earlier levels: a metabolic trajectory bent back toward health must be watched and maintained, or it will bend again. Deployed here, predictive diagnostics becomes an instrument of surveillance as much as of discovery.
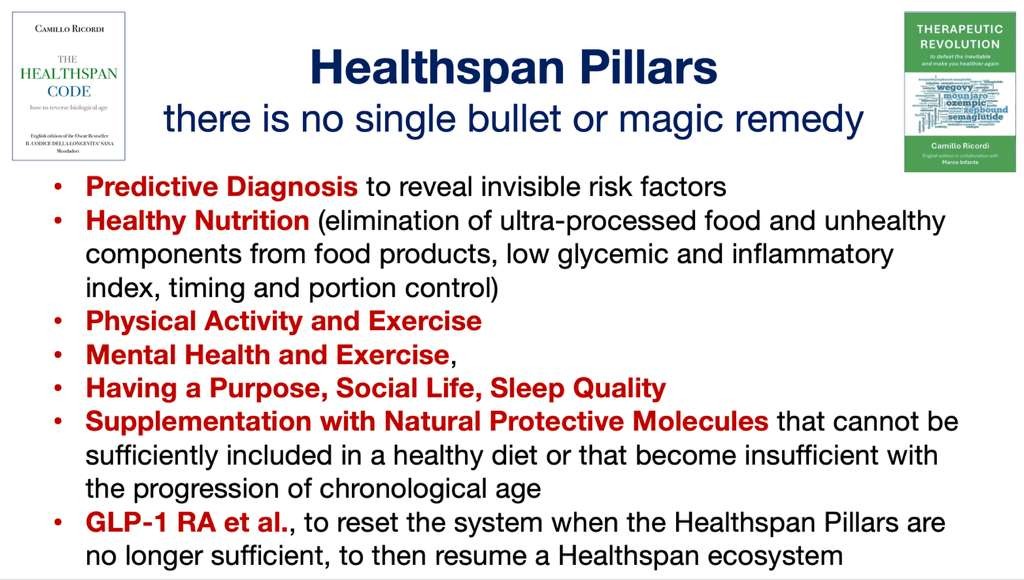
No Single Bullet: An Ecosystem of Pillars
The most seductive idea in modern medicine is the single bullet—one pill, one injection, one edited gene that dissolves a chronic disease. For the epidemic of age-related chronic illness, it does not exist, and the persistent search for it is itself part of what keeps medicine reactive. Healthspan is not prescribed; it is built. It emerges from an ecosystem of mutually reinforcing pillars, none sufficient in isolation and each amplifying the others.
Nutrition. Dietary pattern is among the most powerful modifiable determinants of metabolic health. Minimally processed, plant-rich diets of the kind studied in Mediterranean populations are consistently associated with lower rates of cardiovascular disease, diabetes, and all-cause mortality, while the ultra-processed diet now dominant in wealthy nations drives the opposite.
Physical activity. Movement is not merely caloric arithmetic. Skeletal muscle is a metabolic and endocrine organ, and its maintenance underlies insulin sensitivity, immune function, and cognitive resilience. Cardiorespiratory fitness, measurable as maximal oxygen uptake, is among the strongest known predictors of longevity, and aerobic and resistance training each contribute independently.
Cognitive and social engagement. The brain, like muscle, follows a use-it-or-lose-it logic. Sustained mental challenge builds cognitive reserve, and rich social connection is a robust predictor of health: chronic loneliness and isolation carry mortality risk comparable to long-established physical hazards.
Sleep and environment. Sleep is when much of the body's repair occurs, including the clearance of metabolic waste from the brain. Chronic sleep disruption degrades metabolic, immune, and cognitive function. Around it sits the broader environment—air quality, chemical exposures, and the chronic psychological stress whose cumulative physiological burden steadily erodes resilience.
Targeted supplementation. Some protective molecules are difficult to obtain in adequate amounts from the modern diet; others are synthesized by the body in quantities that decline with age. Where a specific, evidence-based deficiency or age-related decline can be identified, targeted supplementation can restore what nutrition alone no longer provides. This is a matter of precision rather than indiscriminate consumption: the aim is to correct identified gaps, not to accumulate pills.
From Reset to Adherence
Finally, when a person is already moving in the wrong direction—when the pillars alone can no longer arrest a dangerous trajectory—pharmacology has an essential role. Its proper purpose is to serve as a metabolic reset: to interrupt a self-reinforcing decline and return the body to a healthspan trajectory from which the pillars can once again take over.
The GLP-1 receptor agonists now reshaping the treatment of obesity and diabetes are the clearest contemporary example, and also the clearest cautionary tale. They are genuinely powerful tools for resetting metabolism. But their benefit is squandered when they are treated as a permanent substitute for the foundations of health rather than a bridge back to them—when patients build no durable habits beneath the pharmacology and relapse the moment the prescription ends. The drug can buy the opening; only the pillars keep it. A serious strategy uses medication to interrupt the wrong trajectory and then deliberately returns the patient to the nutrition, activity, sleep, and engagement that sustain health. Reengagement, not dependence, is the objective.
One Health: You Are Only as Healthy as Your Surroundings
Even the most disciplined personal effort has limits, because no individual's health is truly individual. This is the premise of the One Health vision: that human health is inseparable from the health of the food system, the environment, and the community that surround it. A person cannot fully engineer their own healthspan while immersed in conditions that steadily erode it. The pillars are never practiced in a vacuum; they are enabled or obstructed by forces largely beyond personal control—the food products that fill the shelves and are engineered to be overconsumed, the quality of the air drawn in with every breath, the chemical and psychological exposures of ordinary life. Together these can constitute what is fairly called a proinflammatory environment: a milieu that pushes the body's baseline toward the chronic, low-grade inflammation that underlies so much age-related disease.
This is not an argument for fatalism. Even within a hostile environment, the tools that anchor this entire model retain their force: risk factors can be identified years before they progress toward disease, and their effects can be measured, monitored, and mitigated. A person who cannot single-handedly change the air of their city can still learn that it is prematurely aging their lungs and arteries, and act deliberately to offset it. But the deeper implication is unavoidable. A serious healthspan strategy is not only clinical but civic: it requires building environments—of food, air, and community—in which health is the default rather than the exception. Individual medicine and collective environmental policy are, in the end, the same project.
One Patient, Four Levels
Consider how this would work for a single, hypothetical individual: a man of forty-five who feels well and carries no diagnosis. Under today's reactive system he is effectively invisible until something breaks. Under a healthspan system, a predictive panel detects early insulin resistance, rising inflammatory markers, and a biological age several years ahead of his chronological one (Level One). Those signals trigger a structured intervention—dietary change, resistance training, improved sleep, correction of a documented nutrient deficiency—that returns his metabolic markers to a healthy range over months (Level Two). Had he instead presented a decade later with established coronary disease, the same system would bring the full weight of advanced cardiology to bear (Level Three). And once treated, he would not be discharged into neglect but monitored and supported to prevent the next event (Level Four). The four levels are not competing philosophies; they are a continuum, and predictive diagnostics is the thread running through all of them.
The Highest-Return Investment
The economic case for reorganizing medicine in this way is not incremental; by credible estimates it is overwhelming. A 2021 analysis published in Nature Aging calculated that a single additional year of healthy life expectancy, achieved across the population by slowing the biology of aging itself, would be worth on the order of $38 trillion, with compounding gains worth far more. No individual drug, device, or hospital expansion offers a return of remotely comparable scale, because those interventions address diseases one at a time, after they occur, whereas targeting the shared mechanisms of aging addresses many at once, before they occur. Prevention, in this light, is not the discretionary remainder of a health budget to be funded after the so-called real medicine. It is the single highest-return investment a society can make in both its health and its fiscal solvency.
Paying for Prevention
If the case is this strong, why does the system not already act on it? Because it is not paid to. Reimbursement in the United States—through Medicare, Medicaid, and the private insurers that follow their lead—is built to pay for procedures performed on people who are already sick. It compensates the treatment of disease richly and the prevention of disease barely, if at all. A cardiologist is reimbursed handsomely for placing a stent in a blocked artery and almost nothing for ensuring the artery never blocks. As long as that asymmetry persists, the most valuable medicine available will remain financially invisible, and predictive, preventive care will remain a boutique service for those who can pay out of pocket rather than a universal standard.
Correcting this is a policy choice, and a tractable one. Payers can begin reimbursing validated predictive diagnostics and early, prodromal-stage intervention on the same basis they now reimburse late-stage treatment. Regulators, including the Food and Drug Administration, can establish clear and rigorous pathways for the diagnostics and preventive therapies the model depends on, so that innovation is neither waved through without evidence nor smothered for want of a route to approval. Public programs can pilot value-based arrangements that reward keeping populations healthy rather than billing for their illnesses. And employers and insurers—who ultimately bear the cost when workers become patients—have every financial incentive to lead. None of this requires weakening American medicine's strengths. It requires paying for the right things, in the right order, at the right time.
The Choice
The United States has spent a generation running an expensive experiment and has produced an unambiguous result: a nation cannot buy health by spending ever more inside a system designed to wait for disease. The tools to build a different system now exist. Predictive diagnostics can reveal risk years in advance; artificial intelligence can make sense of it at scale; a substantial body of evidence defines the pillars that sustain health; and pharmacology, used wisely, can reset those who have drifted off course. What remains is the decision to organize and finance medicine around preventing disease rather than merely reacting to it. The question is not whether we can afford to make that shift. Given $5.3 trillion spent and a last-place result, the only serious question is whether we can afford not to.
References
1. World Health Organization, Global Health Observatory. Healthy life expectancy (HALE) at birth, most recent available estimates (2022–2024) (indicator WHOSIS_000002, both sexes). data.who.int.
2. OECD, Health at a Glance (health expenditure per capita, PPP international $, 2022–2024); and WHO Global Health Expenditure Database via the World Bank / Our World in Data (2022–2024 figures for Singapore, UAE, and Saudi Arabia). Healthspan efficiency index is the author's own analysis combining references 1 and 2.
3. Centers for Medicare & Medicaid Services, National Health Expenditure Data, 2024 (U.S. health spending $5.3 trillion; ≈18% of GDP).
4. International Diabetes Federation, IDF Diabetes Atlas, 11th ed. (2025): 589 million adults with diabetes in 2024, projected 853 million by 2050.
5. Scott AJ, Ellison M, Sinclair DA. The economic value of targeting aging. Nature Aging. 2021;1:616–623.
6. World Health Organization, Global Health Estimates: life expectancy and healthy life expectancy, 2000–2024 (context for HALE trends).
Camillo Ricordi, M.D., is a professor of surgery at the University of Miami Miller School of Medicine and a Fellow of the National Academy of Inventors.
Disclosures: [to be added by author]















Comments